
WHY HAE
REQUIRES
LIFELONG
MANAGEMENT

HAE Is a Genetic Condition
While there is no cure for HAE, treatments help manage the condition.
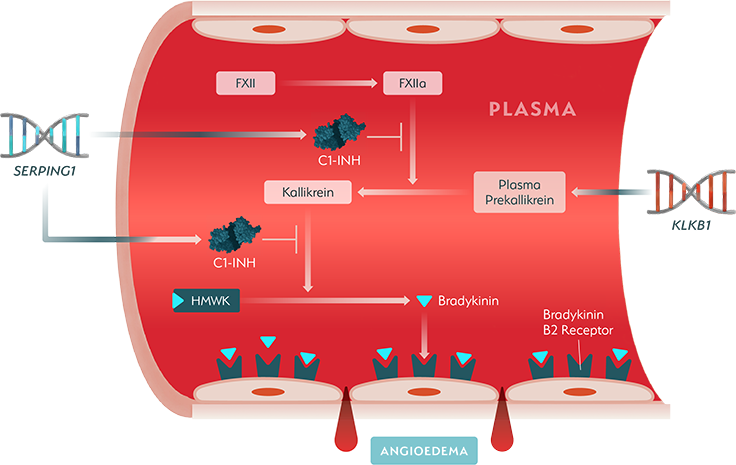
Overproduction of bradykinin leads to swelling attacks, which can occur via multiple pathways in patients with Type I and Type II hereditary angioedema (HAE). A key pathway is the kallikrein-kinin system.1-5

The Kallikrein-Kinin Pathway
The kallikrein-kinin system ultimately produces bradykinin. This process is initiated when Factor XII activates to Factor XIIa. This converts plasma prekallikrein, which is made according to instructions from the KLKB1 gene, to kallikrein. Kallikrein then cleaves high-molecular-weight kininogen (HMWK) to release bradykinin. Bradykinin increases vascular permeability, promotes vasodilation, and activates sensory nerves. In people without HAE, the pathway is tightly regulated by C1 esterase inhibitor (C1-INH).1-5
C1-INH Dysregulation and HAE
Type I and Type II HAE are caused by mutations in the SERPING1 gene, leading to dysfunctional or low levels of C1-INH. This results in uncontrolled feedback activation of Factor XIIa and kallikrein, and subsequently overproduction of bradykinin, causing blood vessels to leak into surrounding tissues in painful HAE swelling attacks.5-7
Approved treatments MAY require repeated lifelong dosing to manage attacks.5-7
Reframe Your HAE Management
Reframing Patient Perspectives
Sign up for more information
that may help your patients living with HAE.
References:
- Bork K, Hardt J, Witzke G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J Allergy Clin Immunol. 2012;130(3):692-697. doi:10.1016/j.jaci.2012.05.055
- Farkas H. Pediatric hereditary angioedema due to C1-inhibitor deficiency. All Asth Clin Immun. 2010;6(1):18. doi:10.1186/1710-1492-6-18
- Mendivil J, Murphy R, De La Cruz M, et al. Clinical characteristics and burden of illness in patients with hereditary angioedema: findings from a multinational patient survey. Orphanet J Rare Dis. 2021;16(1):94. doi:10.1186/s13023-021-01717-4
- Banerji A, Li Y, Busse P, et al. Hereditary angioedema from the patient’s perspective: A follow-up patient survey. Allergy Asthma Proc. 2018;39(3):212-223. doi:10.2500/aap.2018.39.4123
- De Maat S, Hofman ZLM, Maas C. Hereditary angioedema: the plasma contact system out of control. J Thromb Haemost. 2018;16(9):1674-1685. doi:10.1111/jth.14209
- Maurer M, Magerl M, Betschel S, et al. The international WAO/EAACI guideline for the management of hereditary angioedema-the 2021 revision and update. Allergy. 2022;77(7):1961-1990. doi:10.1111/all.15214
- Wedner HJ. Hereditary angioedema: Pathophysiology (HAE type I, HAE type II, and HAE nC1-INH). Allergy Asthma Proc. 2020;41(Suppl 1):S14-S17. doi:10.2500/aap.2020.41.200081